| 緊急警告!うがい・手洗い・マスクではインフルエンザは防げない | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| HOME |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
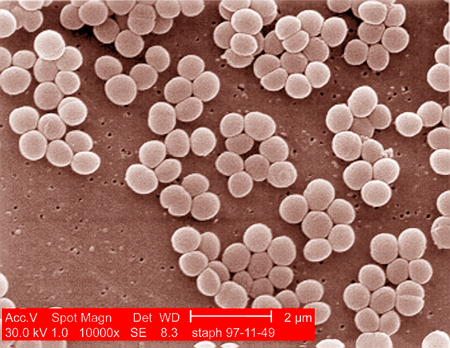
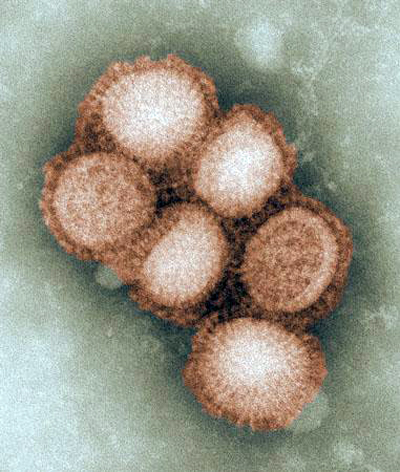 新型インフルエンザウイルスの電子顕微鏡写真 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ウイルスの大きさは 20~970nm(1mmの100万分の1)で、細菌の大きさの1~5μm(mmの1000分の1)と比較すると、格段と小さいことが判ります。また殆どのウイルスは 300nm 以下と小さく、黄熱ウイルスが 40~50nm(μm の1/1000) ノロウイルスは 25~35nm と極端に小さくなります。これは電子顕微鏡無しでは絶対に見ることができません。因みに光学顕微鏡の限界は 200nm 、肉眼での視認限界が凡そ 0.01mm とされています。 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ネット上には「うがいと手洗い」よる感染症予防を奨励するサイトが満ち溢れています。記述内容に医学的根拠(エビデンス:Evidence-Based Medicin)は存在するのでしょうか。 「風邪は万病の元」とも言われ、私たちの体に起こる怖い変調の一つです。ましてやタミフル等の抗生物質も効果がない最近の強力なインフルエンザウイルスに対して果たして有効なのでしょうか。 「うがいと手洗い」を奨励するサイトの趣旨は、口腔内や手の表面に付着した菌を「ただ洗い流すだけ」の一言に尽きます。確かに多くの病原菌は、喉や消化器官、目、鼻等の粘膜から感染します。「うがいや手洗い」は付着した汚れ(菌)を洗い流すには「ある程度の効果」は望めるでしょう。然しながら、インフルエンザは細菌感染ではなくウイルス感染によって引き起こされます。ウイルスは細菌ではありません。生物学上は非生物で、自分で増殖することができません。従ってウイルスは生体の細胞に寄生し、その細胞内でのみ増殖が可能になります。仮にウイルスが1個侵入すると、8時間後には最低でも100個、16時間後には1万個以上、24時間後には100万~数千万個に増殖すと云われています。そして何とも厄介なのは、細菌感染に有効な抗生物質もウイルスには全く効果がないことです。 「うがい」はウイルスを細菌と誤解したことから起きた「都市伝説」のような「たわごと」です。その点「手洗い」は納得がゆく効果的な手段と言えます。然しながら、この手洗いもウイルスが手にのみ付着しているのだとしたら、絶大な効果を発揮するでしょうが、手は体の極一部でしかありません。実際に露出している部分はその何倍もあり、頭髪や被服にも付着します。強力なエアーシャワーでも浴びた後の手洗いならともかく、ウイルスが付着したと思われる極一部を洗浄するのでは予防の効果は期待できません。 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
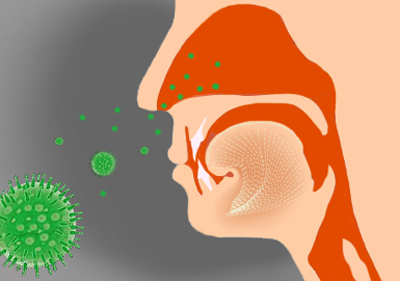
| インフルエンザはウイルスが喉や鼻の粘膜(受容体・レセプター)に付着することで感染します。つまり、インフルエンザウイルスは気道の粘膜にしか感染できず、このインフルエンザウイルスに対応するレセプターは気道粘膜上皮にしかありません。人は口ではなく鼻で呼吸するのが普通です。一旦ウイルスがこのレセプター付着すると、20分程で体内に取り込まれてしまいます。「うがいや手洗い」を奨励すつサイトでは何故かこのウイルス感染の入り口の「鼻腔」が完全に抜け落ちています。また、残念ながらうがいでは気道粘膜上皮にあるレセプターには届きません。 更に、これらの記述が疑わしいと思われる根拠は、「うがいや手洗いがインフルエンザウイルス感染の予防に有効」とするエビデンスが見当たらないことです。医師会や医師が「うがいと手洗い」に関してコメントしているものも多数ありますが、「うがいと手洗い」がインフルエンザウイルスの感染を予防するとの証拠は提示されていませんし、その根拠すら示されていません。 ただ医師としては尋ねられたら、「効果が期待できます」としか言いようがないのかも知れません。インフルエンザは蔓延して、終息するものなのだと理解すべきなのです。 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
●インフルエンザ菌(Haemophilus influenzae)とは、主に呼吸器や中耳に感染する細菌の1種である。インフルエンザという名称が付けられてはいるが、インフルエンザの病原体ではない。 出典: フリー百科事典「ウィキペディア」 「うがい」に関してはココ→ http://square.umin.ac.jp/massie-tmd/majinai.html |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 「うがい」の語源となった鵜飼いの様子 長柄川の鵜飼い(木曾街道六十九次) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
「うがい」の語源は日本の伝統漁法の「鵜飼い」にあります。「鵜飼い」の鵜(う)に魚を飲み込ませ、その後これを吐き出させる様が似ているので「うがい」と呼ばれるようになったとされています。 「うがい」は平安時代から行われてきた習慣で、世界各地にも古くからこの習慣があるようですが、上を向いてガラガラはどうやら日本だけのようで、他の国の「うがい」の目的は主に口臭対策のようです。 古代ローマでは朝起きた時や食後に尿で「うがい」をしたという話しがあります。考えてみれば、健康な人の尿は無菌(出たてのフレッシュな状態)でアンモニア臭もありません。アンモニア臭は尿の成分である「尿素」が空気に触れアンモニアに分解することによって発生します。 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2009年1月21日の深夜(日本時間)に行われた、アメリカ合衆国の大統領就任式の中継を、眠い目をこすりTVでご覧になった方は多かったと思いますが、集まった群衆を見て何か気づかれなかったでしょうか。あれ程多くの人々が集まっているにもかかわらず、誰も(いたのかも知れませんが…)マスクをしていません。これが日本なら、正面から映した映像には多くの人々が白いマスクを着けている様子が映る筈です。このマスクを着けた姿は、諸外国の人にとって朝のラジオ体操同様に奇異に感じる景色の筈です。欧米でのマスクを着用は、その大きな目的は大気汚染による有害な化学物質や飛散する花粉等から身を護るためで、インフルエンザ・ウイルスの防御目的ではないからです。 マスクは微小な粒子(ウイルスを含む)が呼吸器内に侵入し、生体に害を及ぼすことを防ぐ目的(コンビニ強盗にも使用されるようですが…)で使用されますが、果たしてどの程度の大きさの粒子を捉えることができるのでしょうか。 対象が微小なので単位はμ(ミクロン)ですが、このミクロンと言う単位は、1967年の国際度量衡総会で廃止されています、一般的にはまだまだ健在のようで、コチラの方が馴染みがあるので、単位はμ(ミクロン)を使用しています。 最初にインフルエンザの感染経路を知る必要があります。一般に感染は①飛沫感染、②飛沫核感染(空気感染)、③接触感染がその経路として考えられています。 ①の飛沫感染は、感染者の咳やくしゃみを近距離で直接浴びた場合の感染で、水分を多く含み、飛沫物質は約 5μm 以上が普通です。咳1回では約10万個、くしゃみ1回では約200万個のウィルスを含む飛沫が放出されます。咳ではその飛沫が2m、くしゃみでは約3m飛ぶとされています。 ②の飛沫核感染は、感染者の水分を含んだ咳やくしゃみが一旦落下したり、付近の物に付着した後に、飛沫核となり空気中を漂い出した状態で、これが2μm以下になると、瞬く間に水分が蒸発して乾燥します。一旦乾燥すると飛沫核となり、長時間空気中を漂うことになります。この状態での感染を飛沫核感染(空気感染)と呼び、飛沫感染とは区別されています。 この現象はウイルスに限らず、空気中を浮遊する全てのものに言えることで、夏場に比べ空気の乾燥している冬場にインフルエンザが蔓延する大きな理由ともなっています。(新型インフルエンザが、夏場に蔓延していることは、大変奇異に感じられますが、それなら気温も湿度も高いブラジルはナンダイと言われると…難題!) そして最後が③の接触感染で、これは感染者の放出した飛沫が付着した電車の手すりやドアノブ等に触れ、その触れた部分(大抵の場合は手)により間接的に感染する場合と、感染者に直接触れる(握手やキス、その他)ことで感染する直接感染があります。普通感冒のライノウイルス感染では、飛沫感染よりもこの接触感染が多いと考えられ、「手洗い」の根拠となっているようです。 では、①と②の場合、マスクは果たしてインフルエンザ予防に効果はあるのでしょうか。一般的に「マスクは顔の一部または全体に被る、または覆うもの」と定義できます。つまりマスクは顔などの露出部分を、飛翔する有害な物質から守り、それらを体内に取り込ませない目的で使用されます。 煙を豪快に吐いて疾走する汽車を知る人もめっきり減った現代ですが、想像だけはできる筈です。汽車がトンネルをくぐる時には乗客は皆一斉に窓を閉めます。何故なら、それを誰かが怠ると、トンネルを出た時に顔がススだらけ、鼻をかむとススで真っ黒と言う悲惨な状態になります。この場合車窓を閉める目的は、煤煙による汚染を防ぐことです。 仮に、この窓がガラスではなく網戸だとしたら、結果は如何なっていたでしょう。そうです、「閉めても閉めなくても何も変わらない」となります。これは煤煙の粒子が網戸の目より小さいからに他なりません。この簡単な理屈が判れば後は何も言うことがありません。 と言うことで、マスクの効果は如何なるものかを見て行きたいと思います。下は現在市販されているマスクの透過性(粒子を捉えられる能力)を表します。効果が全く期待できないガーゼマスクと、簡易型の使い捨てタイプの紙マスクは除外してあります。 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
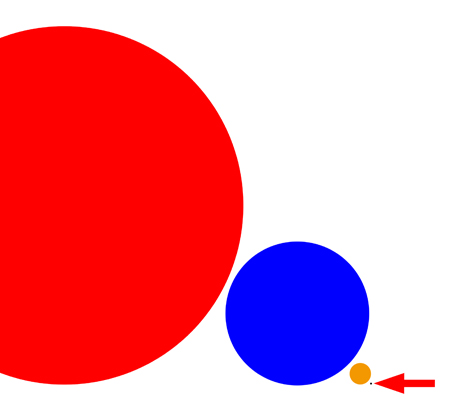 ●が感染者が咳やくしゃみで放出する5ミクロンの飛沫微粒子 ●が乾燥した飛沫の核(空気感染や接触感染を引き起こす)の微粒子で2ミクロン ●が医療用に使われるN95マスクが捕捉できる0.3ミクロンの微粒子 ●がナノマスクが捕捉可能な0.03ミクロンの微粒子(矢印の先の黒い点ですが見えますでしょうか) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| ①の市販マスクの主流を占める不織布製のマスクは、捉えられる微粒子が5ミクロン以上ですので、感染者が「他の者に迷惑をかけない」と意味に於いては、ある程度の評価はできますが、全ての飛沫が5ミクロン以上と言う訳ではないので、予防と言う意味での効果は期待しない方が良いでしょう。また、直接の飛沫感染をかろうじて防げても、飛沫核による感染には全くの無力ですので、インフルエンザ予防の観点からすると、効果なしと言わざるを得ません。 ②の医療用N95マスクは、飛沫感染は確実に阻止できますが、飛沫核による感染にはこれも無力のようです。ほぼ全てのインフルエンザ・ウイルスが 0.3 ミクロン以下だと言う事実を知るべきです。 ③のナノフィルタのマスクは、 0.027 ミクロンまでのウイルスを 99.99% 補足できるといわれています。N95規格のマスクが 0.3 ミクロンまでですので、画期的な能力アップと言えます。 然しながら、全てのマスクが感染者からの飛沫感染を効果的に阻止できたとしても、浮遊するウイルスや、皮膚や髪の毛、被服に付着したウイルスからの間接感染は防ぎようがありません。いくら厳重な防御策を講じても、体全体を覆わなければ意味がないのです。 帰宅後にエアーシャワー室で付着したウイルスを完璧に除去できるならともかく、マスクの装着程度では大した効果は期待できません。つまりは、単独で単純な防御策は全く意味が無いことになります。 幾ばくかの効果を期待しても、それは飛び散ったウイルスの極一部でしかないことを知るべきです。インフルエンザ予防は個人レベルでの努力は、悲しいぐらい無力で意味がありません。 せめて、感染したら他人に害を及ぼさないように、まめに手洗いをして、外出時は医療用マスク、またはナノマスクを装着し、ひたすら人ごみを避け、周囲の物には触れないような努力が必要です。 インフルエンザは蔓延してから終息します。何よりも日頃からの体力が勝負となります。感染後の発熱は、生体が自らを護る為に起動する防御反応で、これはウイルスを殺す効果的な方法なのです。ウイルスは約40℃で死滅します。因みにヒト細胞の死滅温度は42℃です。やはり体力勝負ですか… |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
下記は全て公開されているもので、WHOが現在どのフェーズを宣言しているのか、また国内では第何段階になっているのかが容易に判断できます。 これ等のページさえチェックしておけばインフルエンザに関する最低限の情報は得られる筈です。(但し、公開される情報は一般報道より多少遅れます。) 政府機関の公開情報は全てデータを蓄積した後に詳細に分析される性質のもので、リアルタイムでの対応は期待できませんが、その分情報が正確だと思われます。 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
厚生労働省: ■ 健康:新型インフルエンザ対策関連情報 ■ 健康:新型インフルエンザに関するQ&A ■ 新型インフルエンザ(豚インフルエンザH1N1)に係る症例定義及び届け出様式について ■ ブタインフルエンザに関するQ&A(保健所用)(暫定版)(PDF:108KB) ■ 医療施設におけるブタインフルエンザA (H1N1)ウイルス感染が確定もしくは疑われる患者の診療における感染制御の暫定ガイダンス (米国疾病管理センターによるガイダンス:仮訳)(PDF:211KB) ■ 豚インフルエンザウイルス(H1N1)に関する米国疾病管理センター Q&A(仮訳)(PDF:178KB) ■ 国立感染症研究所 感染症情報センター<ブタインフルエンザ> ■ WHO: Current WHO phase of pandemic alert ■ WHO: Swine influenza 外務省: ■ 海外安全ホームページ ■ 海外安全ホームページ:感染症(SARS・鳥インフルエンザ等)関連情報 ■ 海外安全ホームページ:各国・地域の鳥・新型インフルエンザ 指定医療機関 / 主な医療機関 官邸: ■ 海外における新型インフルエンザの発生に関する政府の対応状況 農林水産省: ■ 新型インフルエンザ対策 ■ 個人・家庭及び地域における新型インフルエンザ対策ガイドライン(PDF:491KB) ■ 新型インフルエンザに備えた家庭用食料品備蓄ガイド(PDF:1,889KB) ■ 米国疾病予防管理センター、略してCDCの公式サイト |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| ウイルス対策をうたったマスクに表示されている効果は限定的だと言う結果が、独立行政法人国民生活センターのテストにより判明しました。商品テストは、市販のマスク15種類を対象に行われ、空気中に浮遊しているウイルスと同程度の大きさの食塩の微粒子をマスクに吹き付け、どの程度その通過を防げるかをテストしたもので、95%以上防げたものは3種類のみで、80~95%と80%未満のものが6種類という結果でした。また、この中で80%未満の6種類のうち3種類は、米国の認定基準の「N95」相当(遮断率が95%以上)を謳っていたにも関わらず、その基準に達していませんでした。
国民生活センターの商品テストで95%以上ウイルスカットが証明されたマスクは以下の3種類でした。 ● 使い捨てフルサポートマスク 販売元:株式会社N&N コーポレーション ● DR.SACCIインフルエンザ立体型マスク 販売元:クー・メディカル・ジャパン株式会社 ● micro CATCH MASKミクロキャッチマスク 輸入元:株式会社シンコー |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| 上記の国民生活センターテスト結果(PDF) → テスト結果 | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 上はブドウ球菌の顕微鏡写真 へそのゴマはブドウ球菌の住み家で~す シッカリ掃除しましょうネ!  |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
細菌の種類と大きさ |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
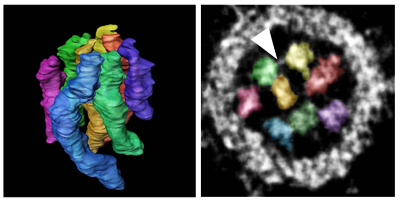
| □ 2012/01/25 ウイルス遺伝子立体構造解明成功 《管理人のブログ So What より》 つい先日、致死率が60%にも達する鳥インフルエンザ・ウイルスの研究成果の発表(鳥から人へ感染する変異体)が一時棚上げになった。生物兵器に利用される恐れがある、との理由でアメリカから横槍が入り60日間一旦発表を控え対策を練るようだ。研究施設がらこのウイルスが漏れ出すようなことでもあれば、全世界の半分が死ぬと云われる恐ろしいウイルスだ。 今朝(25日)は、東京大医科学研究所や兵庫大などの研究チームが、インフルエンザウイルス(A型H1N1亜型)粒子内の立体構造を視覚化することに成功したとのニュースが飛び込んできた。 《 続きは管理人のブログで → So What #016 ウイルスと湿度・温度との関係 2010/12/18 》 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| ストリーマ放電技術による「新型インフルエンザウイルス」 への効果実証 | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| ダイキン工業(株) ベトナム国立衛生疫学研究所と共同実証 実験結果ダウンロード PDF | |||||||||||||||||||||||||||||||||||||||||||||||||||||
 2009年9月16日 新型インフル100%除去 ダイキン、空気清浄で実証 ダイキン工業は15日、空気清浄の独自技術「ストリーマ放電」が新型インフルエンザウイルスを100%除去できることを実証したと発表した。ウイルスに照射すると、4時間で完全に除去できたという。新型インフルエンザをめぐっては、三洋電機が電解水を使った同社の空気清浄技術で感染力を99%抑制する効果があると発表するなど、各社が「性能」を競い合っている。 ダイキンは、ベトナム国立衛生疫学研究所と共同で実験を行った。実験では、ウイルス培養溶液に照射したあと、細胞に接種して7日間培養。ウイルスの残存状態を調べた。4時間照射した場合、細胞から完全にウイルスを除去したことが確認できたという。 ダイキンは5月には同研究所と共同で、ストリーマ放電が鳥インフルエンザウイルス(H5N1型)を3時間で除去できることが確認できたと発表している。ダイキンはストリーマ放電を家庭用の空気清浄機3機種に搭載しており、今回の実証結果をアピールしていく考えだ。 (2009年9月16日 08:41) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
2009年9月15日 ダイキン工業株式会社は、ベトナム国立衛生疫学研究所のレ・ティ・クイン・マイ博士(以下、マイ博士)との共同研究により、強力な酸化分解力を持つ当社独自のストリーマ放電技術が、現在世界中で猛威を振るっている「新型インフルエンザウイルス:A型 H1N1※1」(以下、新型インフルエンザウイルス)を4時間で100%分解・除去することを世界で初めて※2実証しました。 ストリーマ放電技術によって、新型インフルエンザウイルスの表面のタンパク質が酸化分解され、感染力を失ったことにより今回の実証結果が得られたと考えられます。 昨今の国内における新型インフルエンザ感染者数の増加により、ウイルスに対する警戒が強まっています。当社のストリーマ放電技術は、本年5月に「強毒性ヒト由来鳥インフルエンザウイルス:A型H5N1」を3時間で100%分解・除去することが実証されたことをはじめ、季節性インフルエンザウイルス、ノロウイルス、食中毒の原因となる毒素や細菌、ホルムアルデヒドなどの有害物質の不活化効果が実証されており、生活を脅かすウイルス感染を予防する技術として期待されます。(ダイキン工業株式会社HPより転載 http://www.daikin.co.jp/index.html ) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 マスク姿で通勤する人たち。人が大勢集まる場所では効果があるとされているが、それでも完全な予防は期待できないようだ=20日、大阪市北区 「マスク」 新型インフルエンザで需要急増 予防効果なし!?「過剰防衛」 2009.5.21 08:03 ■効果の認識 国内外でズレも 新型インフルエンザの感染拡大で、マスク姿の人があちこちで目立つ。手のアルコール消毒に加え、マスクの着用を求めるケースもみられる。しかし、日本などアジア諸国で見られるそのマスク姿も、欧米ではほとんど見られない。「予防対策にはマスク」という衛生習慣を持つ日本との認識のズレか。それともマスクには予防効果がないのか-。(森本昌彦、小川真由美) ■「格好悪い」 都内に住む女性会社員は4月27日から30日まで、仕事で米ニューヨークに滞在。4日間、地下鉄とバスで、5番街やタイムズスクエア、マンハッタン南部のウォール街やソーホー地区などを訪れた。繁華街のほか、買い物客で混雑する人気衣料品店、有名レストランにも足を運んだが、マスクをしている人は皆無だった。 滞在中、朝のテレビ番組では連日、新型インフルエンザ関連のニュースが流れていた。しかし、感染の広がりの端緒となった都市とは思えないほどの平静さに驚いた。予防のため、日本からマスク5枚を持参したが拍子抜け。ニューヨークで働く米国人男性は「怖がる必要はない病気でしょ。マスクは格好悪いからしていない」と、いたって冷静だった。 逆にマスク姿を笑われる事もあった。マンハッタン南部からブロードウェーへ続く地下鉄に乗ったとき、地下鉄構内の空気が悪かったため、マスクをしていた。すると、前に座っていた少年が自分を見て笑う。その笑い声で車内の他の乗客からも視線を向けられ、思わず「インフルエンザに感染したと思われたかも」と焦った。 「インフルエンザじゃないよ」と話しかけると、「マスクが鳥のくちばしみたいで面白い」と返ってきた。 ■教育の差 新型インフルエンザがこれだけ世界に)蔓延(まんえん)しているにもかかわらず、なぜ欧米ではマスク姿の人がいないのか。新型インフルエンザに詳しい元小樽市保健所長の外岡立人さんは「インフルエンザ予防のため、マスクをするのは日本とアジアの一部の国で定着している衛生習慣」と指摘する。 その理由として、外岡さんは「欧米では、自分への感染がマスクで防げるかどうかについてはっきりとした効果があるとされておらず、マスクは病原体を持っている人が第三者にうつさないために使用されている」と説明。欧米では、手にウイルスがつくことが考えられるため手洗いをしたり、人込みに入らないようにしたりする教育が徹底的に行われている。 つまり、欧米でマスクをしている人は「自分が病気で第三者にうつさないためにしているか、顔を見られたくないためにしている」(外岡さん)という。 ■発症したら外出控える 予防アイテムとして、マスクの効果はどうなのか。新潟大学大学院の鈴木宏教授(公衆衛生)は「第一義的には(新型インフルに)かかった人が他の人にうつさないことに効果があり、自分に感染するのを完全に防ぐものではない」と指摘。さらに、「マスクを外すこともあり、鼻や口を完全に覆っていないなど正しい付け方をしていない人もいる。それより、せきをしている人が外に出ないようにすることが効果があるのではないか」と分析する。 多くの人がマスクをつけて生活している日本。鈴木教授は「街中にウイルスがウロウロしているわけでもなく、みんなが(新型インフルエンザ)にかかるわけでもないのにマスクをしている人が多いのは過剰防衛に映る」。 人が大勢集まる場所などでは効果があるとされているが、それでも完全な予防は期待できない。手洗いをしっかりするなどの予防を行い、仮に感染が疑われる症状が出たら拡大を防ぐためにマスクをすることが大事のようだ。 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| 今冬のインフルエンザ総合対策について(平成20年度) PDFです | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| ■ オセルタミビル(商品名:タミフル)耐性のインフルエンザウイルスについて (厚生労働省 報道発表資料 2009年1月) | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
■ 市民のための新型インフルエンザ対策ガイドライン 第1版 PDFです H5N1鳥インフルエンザから新型インフルエンザへ 市民の新型インフルエンザに対する備え 観光地域における対策 小樽保健所 平成19年5月 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| ■米国CDC:新型インフルエンザ感染予防のための一般市民の医療用および高機能マスク使用に関する暫定的勧告 | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|
This document provides interim guidance for the use ofrespirators and facemasks by individuals and families during aninfluenza pandemic. It was developed from existing U.S. Department ofHealth and Human Services guidance for the use of these devices in non-occupational community settings, posted on the internet at http://www.pandemicflu.gov/plan/community/maskguidancecommunity.html.While we do not have sufficient data to make science-basedrecommendations regarding every aspect of facemask and respirator use,individuals and families have requested additional information to assist in their pandemic influenza preparedness plans. During an influenza pandemic, one maybecome ill following close contact with someone who is infected athome, in the community, at work, or at school. The best ways to reducethe chance of illness are to avoid crowded settings, reduce close contact with others (within about 6 feet), and practice good hygiene (handwashing and covering coughs and sneezes). Using protective measures in workplaces, reducing contacts among children by closing schools, and canceling public gatherings also are likely to further reduce the risk of infection if these measures are used in the event of a severe pandemic. Facemasks and respirators may further decrease, but will not eliminate the chance of becoming infected, so their use does not lessen the importance of reducing close contacts and improving hygiene: the best protection can be achieved by combining several measures, each of which will partially protect against pandemic influenza. Afacemask or respirator, if used correctly, may reduce the risk ofacquiring or transmitting pandemic influenza illness in certainsituations. Although the actual benefit of facemasks or respirators in preventing influenza transmission is unknown, use in certain situations may be warranted during a pandemic. If entry into a crowded setting is unavoidable (e.g., mass transit or going to a crowded store to purchase essentials such as medications), a facemask should be used, both to protect the wearer’s nose and mouth from other people’s coughs and sneezes, and to reduce the wearer’s likelihood of coughing or sneezing on others. A respirator should be used by individuals for whom close contact with an infectious person is unavoidable, such as when caring for a sick household member. Key messages: The first and mostimportant steps in reducing one’s risk of pandemic influenza are tolimit close contact with others as much as possible and to practicegood hygiene. These measures should be used at all times, regardless of whether a facemask or respirator is worn. When a person cannot avoid being in a crowd during aninfluenza pandemic – for example, because they must commute to work onpublic transit – but has no specific expectation of encountering a sickperson, they should use a facemask. When it is necessary to have close contact with someonewho is ill with pandemic influenza – for example, to give care to afamily member – one should use an N95 respirator or equivalentcertified by the National Institute of Occupational Health and Safety (NIOSH) and consider specifically using a respirator model that also is cleared by the U.S. Food and Drug Administration (FDA) for use by the general public in public health medical emergencies. Ill persons should use a facemask when they must be in contact with others. A facemask (for example, a surgical mask) is a disposable mask thatcovers the nose and mouth. When used properly, facemasks may helpprotect against influenza by blocking droplets – created when someonecoughs or sneezes nearby – from reaching the wearer’s nose or mouth. If someone who is infected with influenza wears a facemask, it will trap their own secretions and may help protect others who are nearby. A facemask also may help keep an uninfected wearer from touching their nose or mouth and potentially infecting themselves with influenza virus that is on their hands. Facemasks are inexpensive and are relatively comfortable to wear. Some small facemasks may fit larger children but children may have trouble wearing them correctly and consistently. TheFDA has cleared many facemasks. These facemasks have been tested toshow that they can trap germs and resist fluids, and will not causeskin reactions or breathing difficulties. FDA-cleared facemasks are labeled to be used by healthcare professionals and generally marketed as medical products sold “over the counter” by medical supply companies. They may be labeled as surgical masks, procedure masks, isolation masks, dental masks, or laser masks. FDA has not cleared any facemasks specifically for use by children. Disposable masks that are not labeled for medical uses are not subject to FDA oversight and their quality is not known. Even if they look similar to facemasks, disposable masks not labeled for medical use, such as those commonly sold at hardware stores, may not provide the same protection against infection. Questions about a brand or type of facemask may be answered by a pharmacist or healthcare provider. General information on buying or wearing facemasks may be found on the FDA website, http://www.fda.gov/cdrh/ppe/masksrespirators.html. Instructions on how to correctly put on and take off a facemask areincluded with the packaging of some products. Correctly removing afacemask so that one is not exposed to contaminated mask surfaces is very important; good handwashing or use of a waterless hand-hygiene product before putting on and after taking off a facemask is critical. An N95 filtering facepiecerespirator is a disposable respirator that covers the nose and mouth. Like a facemask, a respirator will trap infected droplets. Inaddition, if worn correctly, it will protect against breathing in small particles that may contain viruses. Respirators, which generally are worn in healthcare and other occupational settings, are tested and certified by NIOSH. NIOSH-certified disposable N95 respirators are marked with the manufacturer’s name, the part number (P/N), the level of protection provided by the filter (e.g. an N95 respirator is certified to filter out 95 percent of the most penetrating particulates), and “NIOSH.”[1] Non-certified respirators are available but their effectiveness has notbeen tested by NIOSH. For questions about a brand or type ofrespirator, consult the NIOSH website, http://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/. Instructions for correctly putting on and taking off a respirator areincluded in the package. As with facemasks, correctly removing anddisposing of the respirator to avoid becoming infected from secretions that may be on the device is important; it is critical that hands be washed or decontaminated with a waterless hand-hygiene product before putting on and after taking off a respirator. A respirator works by fitting snugly against theface, forcing inhaled air to come through the filtering material. Inworkplaces where most N95 respirators are used, they are “fit tested”to assure that air does not leak around the sides of the respirator. Although fit testing programs generally are not available for the public, selecting an appropriate respirator, carefully following instructions for its use, and making sure that it fits tightly against the face are critical to ensuring the respirator provides protection. Facial hair or other items that interfere with a close fit will diminish effectiveness. FDA recently cleared the first respirators specifically intended for use by the general public during a public health medical emergency such as a pandemic. These respirators, which also are NIOSH-certified, have directions that are written for untrained users and were tested to show that adult users with a variety of facial sizes could obtain a protective fit using those instructions. Their labeling instructions address the other precautions also needed for the safe use of respirators during an influenza pandemic such as handwashing, proper storage before use, and proper disposal after use. Where these are available, they may be the best option for users without access to fit testing. No respirator, however, will fit all users and one may want to purchase several sizes or models to see which fits best (i.e., fits snugly against the contours of the face) before purchasing a larger quantity. There are no respirators designed for use by children. Because the material used to make respirators is denser than that used in facemasks, it may be more difficult to breathe through a respirator. Persons who have heart or lung disease or other illnesses that affect their breathing should consult a healthcare provider before using a respirator. The effectiveness of both facemasksand respirators is reduced after they are worn for a long time andbecome saturated with moisture, or if they are torn or disfigured. Atsuch times, they should be replaced. They can also become less comfortable to wear and may be more difficult to breathe through after extended use. Because the best ways to prevent influenza infection are to avoid crowds and reduce close contacts with others, there should not be a need to wear facemasks and respirators for long periods of time. In addition the facemasks and respirators should be removed when the wearer is no longer in a setting where close contact will occur. Never wash or disinfect disposable facemasks or respirators and never share used facemasks or respirators with others. Settings where respirators and facemasks should be used will depend on the potential for exposure to infectious persons: A facemask is recommended when exposure in a crowded setting occurs with persons not known to be ill. An example would be exposure on a crowded bus or subway while commutingto work during a pandemic. Because ill persons are advised to stayhome during a pandemic, contacts in most public settings will be with persons who are not ill. However, it is prudent to wear a facemask because one may encounter people who are infectious but not yet ill. A facemask also is recommended for use by ill persons when they must be in close contact with others. The facemask will trap the wearer’s secretions and reduce the risk toother persons. Close contact between ill persons and others should belimited as much as possible. However, such contact will occur when the ill person is being cared for at home or if they need to leave home to access medical care or manage other necessities. Ill persons do not need to wear a facemask when they are not in close contact with others A respirator is recommended for use in settings thatinvolve close contact (less than about 6 feet) with someone who hasknown or suspected influenza illness. In non-occupationalsettings, the most common use for a respirator would be in a householdwhere someone has influenza. One person should be responsible fortaking care of the ill individual and that person should wear a respirator during those contacts. The Centers for Disease Control and Prevention (CDC) will be issuing guidance on home care of an ill person, which will be posted on the internet at www.pandemicflu.gov. Families can use this guidance as the basis for making decisionsabout purchasing respirators and facemasks as part of householdpandemic preparedness. Although not all households will have someonewho becomes ill with influenza during a pandemic, because one cannot predict in which households an infection will occur, it would be reasonable for each household to stockpile some respirators that can be used, if needed, when caring for an ill family member. With proper precautions, a single caregiver can use the same respirator several times over a day for brief care visits with the same ill person in the household,[2]so a stockpile of 20 respirators per household would be reasonable. Decisions on stockpiling facemasks and the number to obtain woulddepend on a family’s situation and their expectation of the need for close contact in crowded settings during a pandemic. Pandemic outbreaks in communities may last 6 to 12 weeks.[3] Persons who cannot avoid commuting on public transit may choose topurchase 100 facemasks for use when going to and from work. Anadditional supply of facemasks also could be purchased for other times when exposure in a crowded setting is unavoidable or for use by an ill person in the home when they come in close contact with others.[4] The cost of a box of 20 N95 respirators is about $15 - $30 and the costof a box of 50 facemasks is about $10 - $20. Therefore, the total costto a family to purchase the recommended number of respirators and facemasks would be about $35 - $70. Becausethe supply of respirators and facemasks is limited, stockpiling onlythe amounts that may be useful during a pandemic and using them onlywhen necessary will help assure that supplies are sufficient for all settings where they are needed: on a daily basis in healthcare and other workplace settings, and for pandemic preparedness among healthcare workers, emergency responders, and others who provide essential services in communities. Stockpilingrespirators and facemasks can contribute to pandemic preparedness inhouseholds but is not the only action that can be taken to prepare. Education on other measures to reduce the risk of being exposed and becoming ill, practicing good habits in handwashing and covering coughs and sneezes, as well as purchasing stockpiles of food and water all are recommended. Several scientific studies currently are being done to investigate the level of protection against influenza that may be provided by respirators and facemasks and the ability of persons to correctly and consistently use these devices. This interim guidance may be modified based on the results from these studies. Additional information on protecting oneself and one’s family in a pandemic is available at http://www.pandemicflu.gov/plan/individual/index.html. -------------------------------------------------------------------------------- [1]It is important to note that other NIOSH-certified N-, R-, or P-filtering facepiece respirators (e.g., N99, R95, and P100) provide anequal or greater level of exposure reduction to airborne particulates as an N95 and can be used if N95s are not available. [2]If a respirator is used several times by a single caregiver for briefcare visits with the same ill person, the outside of the respirator maybecome contaminated with secretions from the ill person; therefore care should be taken to keep the respirator away from other household members between uses and to wash hands well after putting the respirator on. [3]Inprevious pandemics, community outbreaks generally have lasted 6 to 8weeks. Effective public health measures to reduce the spread ofinfection in communities (“community mitigation”) may reduce the overall severity of the pandemic outbreak but could lengthen its duration, potentially to 12 weeks. [4]Facemasks and respirators should be stored in a dry, cool location, andprotected from moisture, insects, dirt and extremes of temperature. インフルエンザ予防におけるマスク着用の意義に関する諸問題:http://homepage3.nifty.com/sank/jyouhou/BIRDFLU/2006/mask.pdf インフルエンザ施設内感染予防の手引き:http://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou01/pdf/03.pdf |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
2009年2月オーストラリアのNew South Wales大学と英国のMedical Research Council Centre for Outbreak Analysis and Modelling at Imperial College Londonの発表によると、 臨床試験の結果、「マスクがインフルエンザや風邪などの呼吸器系の病気から身を護ることができるかも知れない」と言う研究結果が発表されました。どのような基準での研究かは詳しいデータが発表されていませんので判りませんが、まずは参考まで…下がその原文です。翻訳には怪しい日本語訳のexcite翻訳をご利用ください。http://www.excite.co.jp/world/ |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
| A face mask may prevent you getting flu, but only if you wear it 22 Feb 2009 | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|
A clinical trial has shown that face masks can protect against respiratory illnesses such as flu and the common cold, but convincing people to wear them is harder. Researchers at the University of New South Wales, Australia, and the Medical Research Council Centre for Outbreak Analysis and Modelling at Imperial College London ran a clinical trial to investigate the effectiveness of masks. They found that adults who wore masks in the home were four times less likely than non-wearers to be infected by children in the household with a respiratory infection. “In a severe influenza pandemic, there may be limited availability of vaccines in the first few months,” said Professor Neil Ferguson, Director of the MRC Centre for Outbreak Analysis and Modelling at Imperial College London and an author on the study. “In that context, masks are a potentially important additional weapon in the public health arsenal.” The University of New South Wales team, led by Professor Raina MacIntyre, recruited more than 280 adults in 143 families in Sydney during the winter seasons of 2006 and 2007. The adults were randomly allocated masks when exposed to a sick child in the household. Less than half of those asked to wear masks reported having done so consistently. However, adherence to preventative measures is known to vary depending on perception of risk and could be expected to increase during a respiratory disease pandemic. The trial results are published this week in Emerging Infectious Diseases, the journal of the US Centres for Disease Control and Prevention. The researchers say the findings have global implications and are particularly relevant to efforts to combat the spread of flu pandemics and other emerging respiratory diseases such as SARS. But while some governments are already stockpiling masks for use in a pandemic, Professor Ferguson said the evidence to support their use in the community has been limited up until now. “This study starts to close that evidence gap. Our work indicates masks may provide substantial protection so long as they are worn consistently and properly.” He went on to emphasise that uncertainties
remain:
“This study represents a first step. More work is needed to look
at the effectiveness of masks to prevent flu infections specifically, to
evaluate their effectiveness in other community and healthcare settings,
and to investigate the factors limiting compliance with mask use. We estimate
that the reduction in risk of catching a respiratory infection for an adult
caring for a sick child, when they adhere to mask use, is between sixty
and eighty per cent. Whether the risk would be reduced by the same margin
in another setting or where there was more than one source of potential
infection requires further investigation.”
The study was funded by the Australian Department
of Health and Ageing.
(Source: Australian Department of Health and Ageing: Ferguson N,
et al. Effectiveness of face mask use to control respiratory virus transmission
in households. Emerging Infectious Diseases: February 2009)
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
 Traditional Japanese colors |
|||||||||||||||||||||||||||||||||||||||||||||||||||||